The Science is Efficient LFG!

When Love Is Built on Secrets
I grew up in a house where questions were liabilities and answers were currency. The two people who were supposed to love me most taught me that safety lived behind closed doors, that money was a riddle, that truth was a privilege I hadn’t earned. That is how you make a child flinch at sunlight. You do not need slamming doors or raised fists. You can do it with omissions, with moving targets, with the quiet insistence that reality is negotiable. That is how you plant post-traumatic stress in a child’s nervous system and call it “normal.”
This is not melodrama. It is neurobiology. When adults withhold safety, consistency, and truth, a child’s developing brain adapts to chronic threat. Stress systems stay switched on. Memory and emotion wiring reorganize for survival. Over time, those changes harden into the operating system of adulthood. I am writing this to hold my parents accountable in the only language they cannot minimize: the language of science. The facts are blunt. Early, unaddressed trauma rewires brain circuits and stress hormones in ways that echo across a lifetime. Harvard’s Center on the Developing Child calls this a “toxic stress” response—excessive or prolonged activation of the body’s stress systems that disrupts healthy brain architecture and other organ systems, increasing risk for disease well into adulthood. Supportive, reliable caregiving buffers this; secrecy and instability do the opposite.
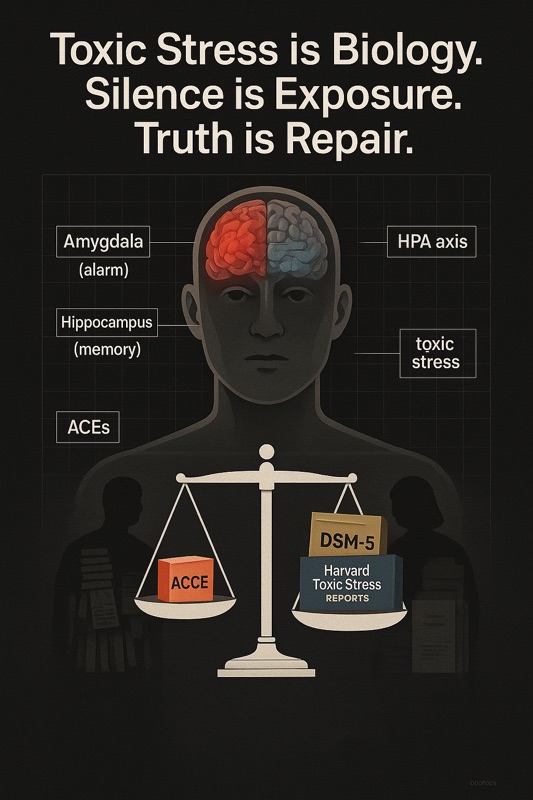
I. Childhood PTSD Is Biology, Not Drama
Start with the amygdala, the brain’s rapid threat detector. In trauma, it becomes hyper-responsive, firing early and often. Neuroimaging consistently shows amygdala hyperactivity correlating with PTSD symptoms; some longitudinal work suggests heightened dorsal amygdala responsivity predicts later trauma symptoms. Translation: if a child learns that the ground can drop at any time, the alarm learns to scream at shadows.
Now look at the hippocampus, essential for memory and context. In adults with PTSD, reduced hippocampal volume is a robust finding across meta-analyses and large studies. The hippocampus is especially sensitive to stress hormones; chronic cortisol exposure alters its structure and function. In some maltreated children, volumes may appear “normal” early, with abnormalities emerging later—an ominous sign that the bill comes due in adulthood. Functionally, this means fractured narrative memory, time collapsing in on itself, the past refusing to stay in the past.
Then the prefrontal cortex (PFC), the braking system—the part that regulates fear, focuses attention, plans, inhibits impulses, and says: “We are safe now.” PTSD is often described as fear dysregulation: the PFC’s regulatory grip is weakened while subcortical alarms dominate. Stress exposure impairs PFC function; in trauma, that imbalance becomes the default. Picture driving with a jammed accelerator and a worn-down brake.
Underneath these regions runs the HPA axis, the stress-hormone cascade. With chronic adversity, the system becomes over-reactive or slow to shut down, priming the body for constant vigilance even in neutral situations. Over time, this leads to maladaptive threat perception and persistent anxiety. This is the physiology of a child trained to scan a parent’s tone for danger because the rules keep changing.
This isn’t a grab bag of correlations. It is a coherent model of how chronic, unresolved childhood stress re-tools the brain for survival at the expense of stability. And it is precisely why I refuse to accept “You’re overreacting” as a verdict on my life. The science says I adapted to the environment I was given.
II. When Parents Choose Silence, They Choose the Child’s Symptoms
There is a public-health framework for the cumulative harm of early adversity: Adverse Childhood Experiences (ACEs). The CDC-Kaiser work shows a graded, dose-response relationship—more ACEs, higher risk of mental and physical illness across the lifespan. Later CDC data replicate the core point: ACEs are common and compound; many children carry several. Silence and secrecy aren’t neutral—they are exposures. They are items on a ledger the body keeps.
Harvard’s toxic-stress model is explicit: without stable, supportive caregivers to buffer stress, excessive activation of stress systems disrupts brain architecture and other organ systems. “Supportive relationships with caring adults” are not poetic extras; they are protective neurobiology. When caregivers lie, deflect, or refuse to provide clarity about safety and resources, they remove the buffer that keeps a child’s physiology within healthy bounds.
In my house, the buffer was missing. Questions about money yielded fog. Boundaries shifted with moods. Explanations arrived late or not at all. That volatility taught my amygdala to overlearn threat and my PFC to waste energy disputing gaslight. This is not me “blaming” my parents for everything. It is me showing the chain of custody between adult choices and a child’s symptoms. The DSM-5 frames PTSD around intrusion, avoidance, negative cognitions/mood, and arousal alterations lasting more than a month after trauma exposure. Gaslighting in the home recruits the same machinery: persistent hyperarousal, avoidance (don’t ask, don’t trigger); negative mood (guilt, shame, distrust); and intrusive re-experiences when a new inconsistency rhymes with an old one.
There is also ICD-11 Complex PTSD—a sibling to PTSD characterized by the core symptoms plus disturbances in self-organization (affect dysregulation, negative self-concept, relationship difficulties), especially after prolonged, interpersonal trauma. Many of us raised in secrecy and instability recognize that profile in the mirror.

III. The Lifetime Bill: Health, Work, Love
The bill for unaddressed childhood PTSD doesn’t arrive as a single diagnosis. It shows up as a pattern: autoimmune flares, metabolic risk, cardiovascular issues, anxiety and depression, substance use, relational volatility, economic instability. Toxic-stress and ACEs research connect early adversity to elevated risks across these domains. It’s not destiny; it’s probability. The mechanism is chronic stress physiology distorting immune, endocrine, and neural systems over years.
This science has given me language for why I freeze before phone calls, why budget spreadsheets feel like interrogation rooms, why compliments land like traps. Hypervigilance is not a personality quirk; it is an amygdala trained by moving targets. Memory gaps aren’t laziness; they are hippocampal scars from too much cortisol for too long. The difficulty trusting “we’re fine now” isn’t stubbornness; it’s a PFC still trying to out-argue alarms wired before I could drive.
Even my whistleblower work sits inside this arc. When you are raised in an atmosphere where facts bend, you either break—or you turn forensic. I learned to document because I had to prove things to people who wouldn’t look. That vigilance found its proper target outside the home, but the trigger pattern is the same: I see, I verify, I escalate. And the same physiology that made me effective also made me exhausted. Trauma’s gift is pattern detection; trauma’s tax is never feeling done.

IV. Accountability, in the Only Terms That Count
So here is the ledger, Mother and Father, keyed to peer-review and public-health consensus:
- Chronic secrecy and inconsistent caregiving in childhood activate toxic stress physiology. Without reliable buffering relationships, stress systems over-activate and fail to shut down, altering brain development and raising lifelong disease risk. This is not theory; this is a central conclusion from Harvard’s Center on the Developing Child.
- PTSD is a disorder of fear dysregulation. The amygdala becomes hyper-reactive, the prefrontal cortex under-regulates, and hippocampal structure/function are compromised; this triad underlies hypervigilance, intrusive memory, and impaired context. This pattern is shown across reviews and meta-analyses.
- ACEs show dose-response harm. The more categories of early adversity, the higher the odds of mental and physical illness in adulthood. This is CDC-Kaiser bedrock and has been reaffirmed in later CDC surveillance.
- Complex, prolonged interpersonal adversity maps to Complex PTSD. ICD-11 distinguishes this condition by adding disturbances in self-organization to the PTSD core. It is what long seasons of relational instability produce.
Notice what is not on this list: “The child overreacted,” “He should get a job and get over it,” “We meant well.” Intent does not cancel physiology. Outcomes are what shape brains.
You often answer my evidence with deflection. You say “everyone has problems,” or “people expose fraud all the time,” as if statistical ubiquity erases biological impact. The CDC’s work says otherwise: common does not mean harmless. Prevalent harms are still harms, and they scale into population-level disease.
You also imply that if there weren’t bruises, there wasn’t trauma. That is scientifically false. The nervous system encodes threat from unpredictability, humiliation, and chronic ambiguity. If your child has to study your face every night to guess which version of you will show up, that is not “household personality.” That is a stress exposure with measurable neural and endocrine correlates.
V. What Accountability Looks Like (and What It Doesn’t)
Accountability does not mean you relitigate every memory with me, trying to win the cross-examination you refused to attend when it mattered. Accountability starts with acknowledging that in our home, secrecy and inconsistency were chronic. That those conditions burden a developing brain. That my symptoms map to those burdens. That you chose not to buffer stress with stability and truth, and the cost landed in my body.
It also means stopping the sabotage of clarity now. When I ask for documentation, produce it—don’t pivot. When I raise health-insurance access or ask for a clean exit plan, deliver it in writing—don’t dangle conditions. In clinical and legal contexts, ambiguity is not care; it is risk. The VA’s and APA’s framing of PTSD is symptom-based, exposure-tied, and time-anchored; it does not ask whether the perpetrator meant well. It asks whether the organism has been overwhelmed and whether symptoms persist. That standard serves children because it centers biology over family PR.
And yes, accountability includes repair. Not with speeches— with buffers. Stable, predictable support. Clear, written agreements. The adult version of what should have been present for the child: consistent, honest, reliable care. That is how you down-regulate a nervous system you helped dysregulate. That is how you put brakes back on the car.
VI. My Terms Going Forward
I am not asking for a perfect past. I am demanding a science-literate present. The facts are on the table:
- My nervous system adapted exactly as the literature predicts for a child raised in secrecy and instability.
- My adult symptoms are not moral failings. They are learned survival responses embedded in brain regions and hormone pathways.
- My boundaries—requests for documentation, written commitments, clean exits—are not attacks. They are trauma-informed design for a livable life.
The work for me is healing: therapy that targets the amygdala-PFC imbalance, practices that restore context and reduce false alarms, environments that reward consistency over crisis. Evidence-based treatments exist, from trauma-focused psychotherapies to skills that strengthen prefrontal regulation—not a miracle cure, but a way back toward a calmer baseline. None of that absolves you. It simply means I am finished letting your deflections author my outcomes.
I am not returning your silence with silence. I am returning it with citations. When you call me dramatic, I will point to the amygdala literature. When you minimize the past, I will bring the hippocampus data. When you say I should “just be normal,” I will show you what chronic cortisol does to PFC control and why “normal” isn’t a switch; it’s a painstaking rebuild. And when you claim everyone has problems, I will hand you the CDC’s dose-response curves and ask whether the population-level disease burden comforts you.
I grew up in a house that taught me the wrong lessons about love: that love hides, that love withholds, that love punishes questions. I reject that curriculum. Love, to a child’s brain, is predictability and truth. Love is a caregiver who answers the same way on Monday and Thursday. Love is a ledger you can read. If you want relationship with me now, it will be built on that definition—not the older one that cost me a decade of sleep.
Coda: The Ledger I Keep
I will not inherit your lies. I will not turn them into my personality. I will not call hypervigilance “who I am” when it is “what happened to me.” The science names the harm. It also names the way home: stable buffers, consistent truth, deliberate regulation. You can join me in that work—or you can keep your myths. Either way, my nervous system belongs to me now, and I am rebuilding it on evidence.




